Vaccines. They’re putting hobbled viruses and bacteria into our system so that they can cause an infection, and thereby build an immunity, right? Like Smallpox and Cowpox, right?
Well, sometimes. That is called a Live Attenuated vaccine. They’re difficult to manage and relatively high risk.
There are many different types of vaccine, all of which involve hobbling the rogue organism to different degrees.
If they get cooked, nuked (that is, sterilized in an irradiation facility such as the one in Upper Hutt), or perhaps killed with strong salt, acid, base, or some such - then it’s called an inactivated vaccine. These are a step up.
They still work, even though the vaccine or bacterium does not cause an infection. They do not replicate in the body. Any reaction that occurs, will be an immune response only. All that means is that your immune system is responding to the foreign matter, like it is when you get a pimple or your hayfever plays up.
A step up again from an inactivated vaccine is a sub unit vaccine. If you, through chemical manipulation, extract just a part of the organism - then you have the safest known approach to creating vaccines today. They are lower in side effects, easier to manage (as there is no live agent to keep alive), although as a real infection does not occur, several shots are needed to provide immunity. If there was a “real” infection, it would provide the body with a steady stream of greeblies to fight.
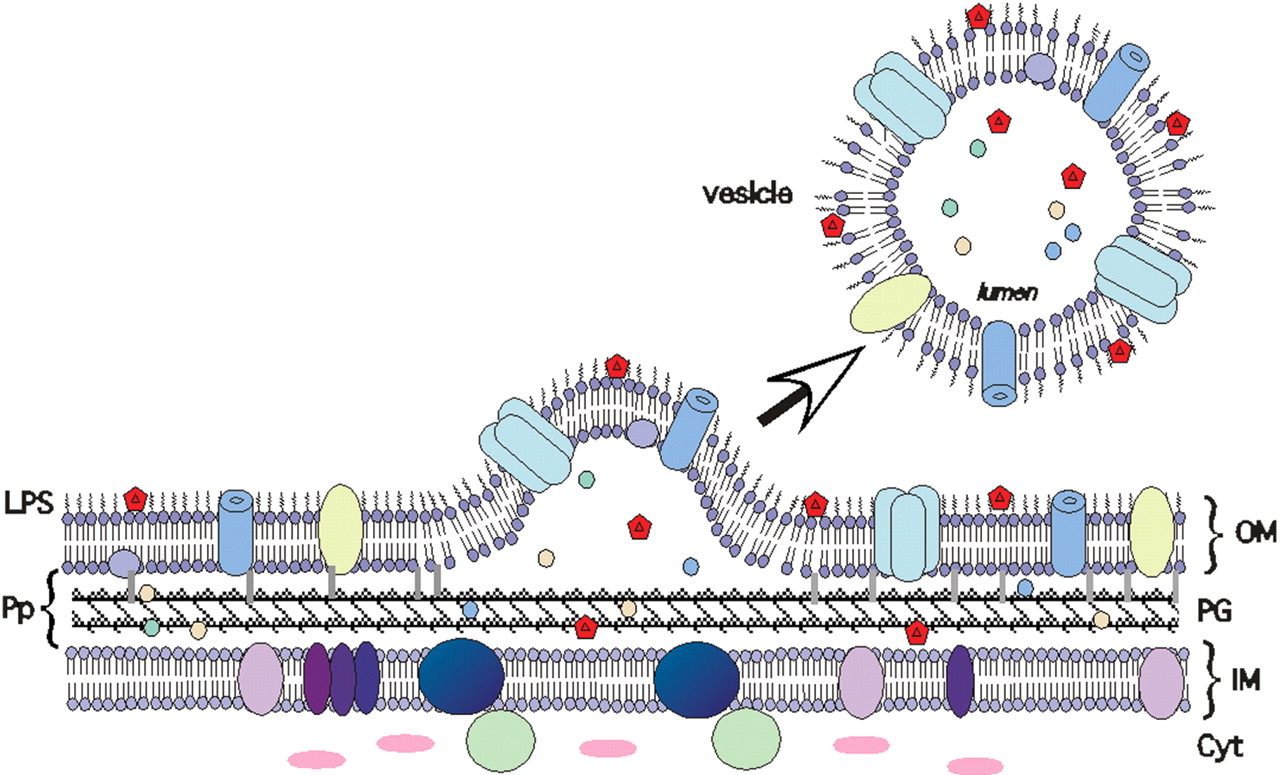
The type of vaccine used for Mengingococcal disease (group B, the type causing NZ’s epidemic since 1991) is called wild-type outer membrane vesicle or wtOMV in the medical literature.
It is something of a testament to the success of modern medical science that society demands almost perfect results from it. But these are relatively early days for the wtOMV approach. It is extremely specific and targeted to a particular strain of a disease. It may not provide indefinite protection; but through testing it can be shown that it can provide protection for long enough to stop an outbreak.
Scientists are working on this. I read with interest the abstract of a paper on the performance of vaccines including MeNZB:
There is good reason to believe that in the coming few years the “OMV-concept” will be exploited further and that a number of cross-protective “universal” antigens will be included in vaccines against serogroup B meningococcal disease.
This is extremely promising. We’re not there yet, and so when vaccines didn’t work 100%, it’s a good idea not to start hating on the scientists or the institutions supporting them. I mean, certainly make them work for their money and stuff but don’t forget that most of these scientists are simply motivated individuals who want to use their talent and skills to make a difference. Look at the far-flung institutes that produced that paper: Norwegian Institute of Public Health, Oslo, Norway; Institute of Environmental Science and Research, Porirua, New Zealand; Victoria University, Wellington, New Zealand; Finlay Institute, Havana, Cuba; Novartis Vaccines & Diagnostics, Siena, Italy; Ministry of Health, Wellington, New Zealand. That in itself speaks volumes about the independence of their work.
Why is the MeNZB Immunity only Temporary?
The full picture of immunity is quite a complex picture; but nonetheless it is well known; one of the things that was certainly very striking to me as I was studying First Year Anatomy & Physiology was the level of detail that science knows. I was quite surprised to know how much information was known, even in the decade-old book I was using as a text.
But basically, immunity is only permanent if it goes through a particular stage of the immune response. I won’t pretend to remember the intricate details, but in essence you don’t get the strongest protection without a real infection, and real infections present the greatest danger - perhaps death with some diseases.
What about averse reactions?
You might already be primed to attack that material being injected to you. You might already have acquired immunity, in which case the reaction will be much more immediate - your system knows these foreign particles and the alarm bells go off. This will cause a reaction.
This is especially the case with N. meningitidis. It is considered normal flora in your throat - 5-15% of people are expected to have it. The throat has an organ called the tonsils which allow the body to prepare itself for infection by fighting the bacteria in the food you eat. So, it’s quite expected that a good number of people will already be immune and therefore elicit a stronger immune response.
But it’s temporary, and links between vaccine responses and autism have been not only debunked but revealed as fraudulent. Don’t let yourself be duped!
What about breast feeding?
For the first 6-12 months of your life, you have antibodies (one mechanism of immune response) floating in your blood which were transferred from the mother. This is called innate immunity, but these antibodies are not transferred via breast-milk; the baby’s digestive system will destroy them before they can!
It’s all a vast Big Pharma conspiracy!
For a start, pharmaceutical companies are probably actually undermining their medium-term takings by producing vaccines. Wouldn’t it be cheaper for them not to produce them at all, and instead sell us remedies when we fall sick?
I have very little time for complaints like this in New Zealand, where there is Pharmac for bulk purchasing power. I just don’t believe that the staff at Pharmac - some of whom I have known and talked to in the past - can be duped by sales execs or that the independent monitoring panels would fail to pick anything up.
That said, I certainly disagree with direct to consumer marketing, and from a macro-economic perspective, the pressure from maintaining high profit margins by our current implementation of capitalism can appear (and often even be) sinister.
The fight against these diseases is the raw fight for existence, which in modern times is already stepping outside of our frames of reference. We need concerted action on this, not half-hearted. It’s a war-scale effort - don’t defect to the enemy!